ACL Injury in Adults
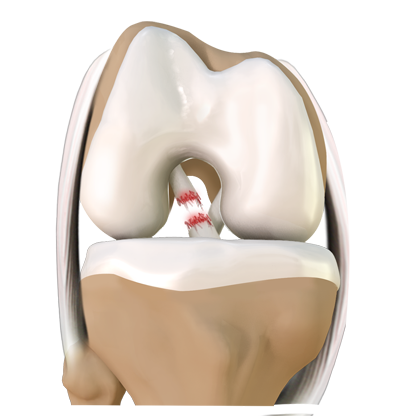
ACL stands for Anterior Cruciate Ligament. It is one of the four main ligaments of the knee joint. It connects the thigh bone (Femur) to the lower leg bone (tibia), which carries the majority of the body weight. On average, the adult ACL is 30 – 33 mm in length and 9-12 mm in width.
It consists of two bundles:
- the anteromedial bundle – it becomes tight during knee flexion and prevents anterior (Front) translation of tibia (shin bone).
- the posterolateral bundle – it becomes tight during knee extension and is primarily responsible for rotational stability.
ACL tear is most common sports related injuries leading to anterior and lateral rotator instability of the knee joint.
Classic history of an ACL injury:
Noncontact deceleration, jumping or cutting action. Other mechanisms of injury include external forces applied to the knee. The patient often describes that the knee has been hyperextended or is being popping out of joint and then reducing. A pop is frequently heard or felt. The patient usually has fallen on the ground and is not immediately able to get up. Resumption of activity usually is not possible, and walking is often difficult. Within a few hours, the knee swells, and aspiration of the joint reveals hemarthrosis. In this scenario, the likelihood of an anterior cruciate ligament injury is greater than 70%.
Causes or Mechanisms of ACL injuries:
Patient need not to have direct trauma to knee for developing ACL tear. Some of the common injuries include:-
1. Deceleration injuries with increased quadriceps contraction:
Anterior force on the proximal part of shinbone mainly caused by severe quadriceps muscle contraction. These kinds of injuries are mainly seen in basketball and football players who suddenly decelerate to change direction.
2. Hyperextension knee injuries:
This mode of injury seen in basketball players (e.g., in rebounding) and in gymnasts during the dismount.
3. Skiing injuries:
The classic cause of knee injury in downhill skiers is a forward fall in which the inside edge of the ski is caught in the snow, placing the knee in external rotation and valgus stress.
4. Trauma:
Direct impact over the lateral aspect of the knee. Patients may hear POP sound at the time of injury.
Symptoms of ACL Injury:
Patient sometimes gives history of feeling “pop” in the knee at the time of injury, pain is diffuse and deep in the knee, swelling and hemarthrosis develop immediately in 70% of cases.
Patient may have feeling of instability which prevents returning back to sports. Some people will have difficulty in weight bearing and some may face problems while using stairs.
Some will have quadriceps avoidance gait (do not actively extend knee), deficiency of full extension secondary to meniscal tears or arthrofibrosis.
Tests for ACL injury:
Anterior Drawer Test
Patient laid supine – hip is flexed to 45 degrees – the knee to 90 degrees – foot placed on the tabletop – foot is stabilized – both hands are placed behind the knee to feel for relaxation of the hamstring muscles. The thumbs are placed on the medial and lateral joint lines. The proximal part of the leg is then gently and repeatedly pulled and pushed anteriorly and posteriorly, noting the movement of the tibia on the femur.

The degreeof displacement in each position of rotation is recorded and compared with the normal knee.
An anterior drawer sign 6 to 8 mm greater than that of the opposite knee indicates a torn ACL.
Lachman Test
This is preferred over drawer test.
Advantages –
- Can be performed in an injured knee without eliciting too much pain
- Eliminates the hamstring tightness
- No restriction from menisci.
The patient laid supine – the involved extremity is positioned in slight external rotation and 30 degrees of knee flexion; the femur is stabilized with one hand, and firm pressure is applied to the posterior aspect of the proximal tibia, which is lifted forward in an attempt to translate it anteriorly.

Anterior translation of the tibia associated with a soft or a mushyend point indicates a positive test result.
Lateral Pivot Shift Test of Macintosh:
Specifically elicits anterolateral rotary instability ofwhich ACL injury is a part. It is used in chronic conditions and is a sensitive test when the ACL has been torn.
With the knee extended, the foot is lifted and the leg internally rotated, and a valgus stress is applied to the lateral side of the leg in the region of the fibular neck with the opposite hand. The knee is flexed slowly while valgus and internal rotation is maintained.With the knee extended and internally rotated, the tibia sub luxates anteriorly. As the knee is flexed past approximately 30 degrees, the iliotibial band passes posterior to the center of rotation of the knee and provides the force that reduces the lateral tibial plateau on the lateral femoral condyle. 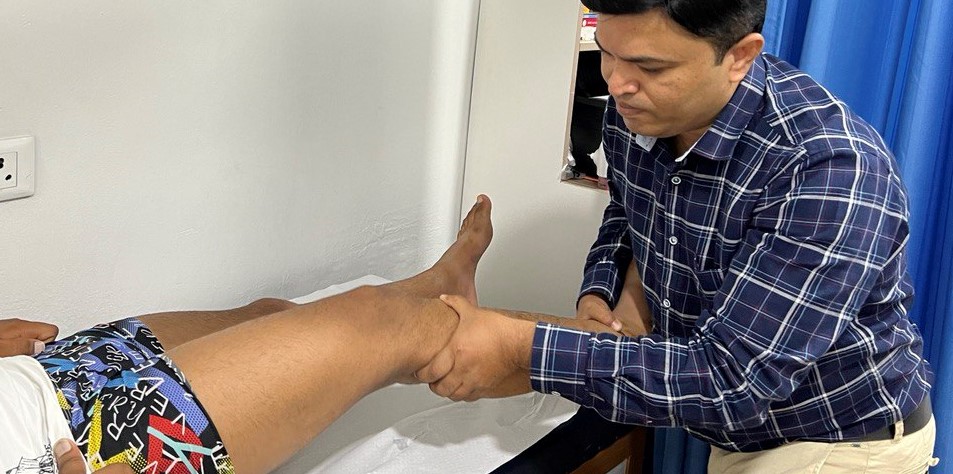
Types of ACL Injury
ACL Sprain (grade 1): They are the most common and mild ones. In this type of sprain, the fibers of the ligament are stretched but not torn. This type of sprain does not require surgery and can be treated by medication, physiotherapy and rehabilitation. Unless treated, the patient suffers from pain, swelling, and difficulty in movement.
Partial ACL tear (grade 2): This is more severe than the previous one because the fibers of ligament are partially torn. In the case of Grade 2 surgery may or may not be required. You need to consult sports injury specialist for proper decision making. 90% cases do not need surgery. The surgery should be done or not also depends on the patient’s age, job, lifestyle and amount of instability and difficulty in moving.
Complete ACL Tear (Grade 3): As the name suggests, in this type of injury, the fibers of the ligament are completely torn. The pain is more severe and so is instability, swelling and tenderness. Surgery is usually required and is done once the swelling reduces. Patient should have at least 90-100 degrees of knee flexion before surgery.
ACL Avulsion Fracture: This is a more severe injury in the ACL than a sprain. In this case, the fiber of the ligament is torn along with a piece of bone, from the part where it meets the bone, the tibia or the femur. This needs emergency surgery to fix the bone fragment to save native ACL. If you delay the surgery, saving your original ACL is not possible and you will need ACL reconstruction in future.
Investigations
MRI is the modality of choice to confirm clinical diagnosis of ACL rupture and evaluate for concomitant pathology.
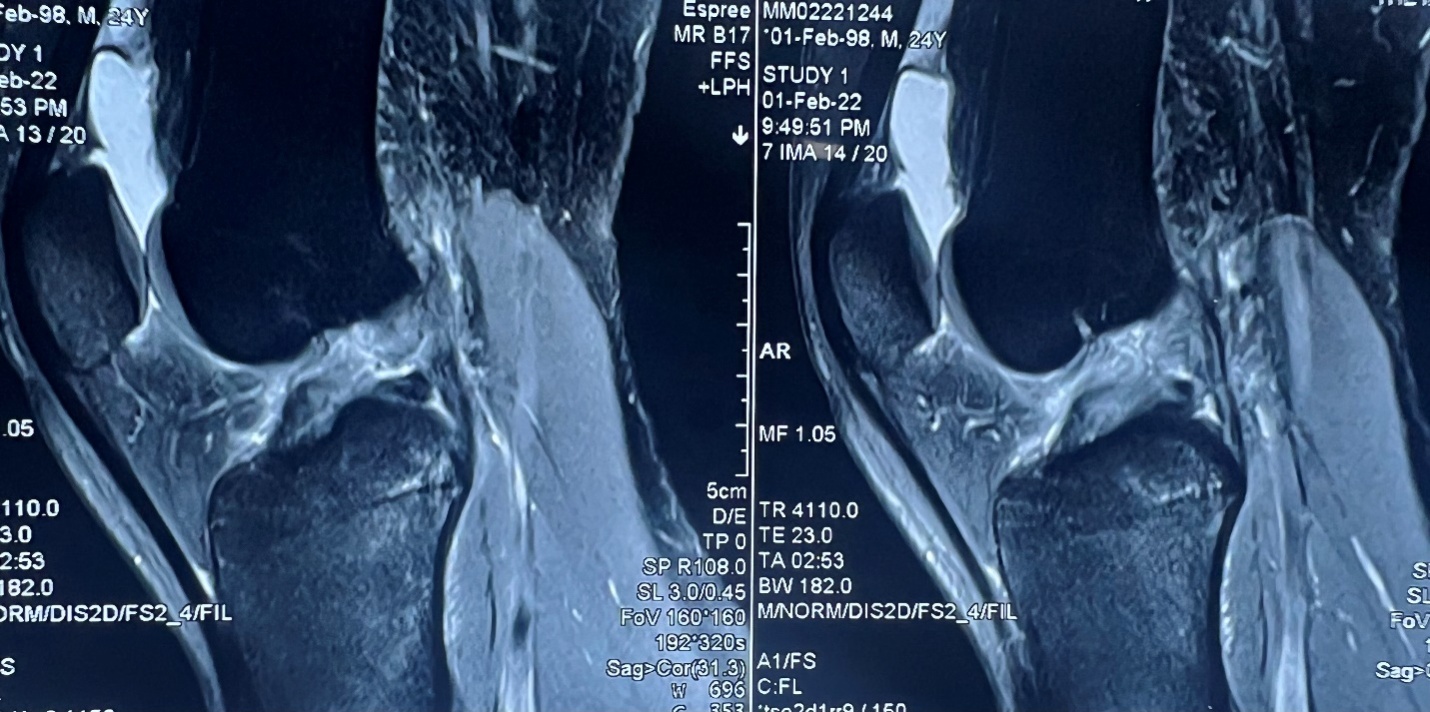
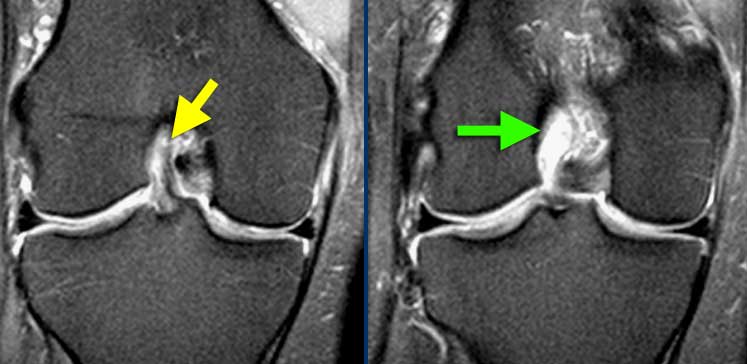
MRI image showing complete ACL tear
Treatment Options:
With the natural history in mind, the surgeon must determine which therapy is most appropriate for a specific patient.
The treatment options – nonoperative, repair of the ACL (either isolated or with augmentation), and reconstruction.
Nonoperative –viable option for who is willing to make lifestyle changes and avoid the activities that cause recurrent instability.
Mainly three factors known at the time of the initial examination correlates with the need for surgery:younger age, pre injury hours of sports participation, and amount of anterior instability.
Nonoperative treatment modes includes Physiotherapy, rest and medications.
https://www.youtube.com/watch?v=11l3l7pXFVY
Indications of ACL reconstrucion
- must have full motion of knee restored following injury (unless meniscal tear causing mechanical block) lack of pre-operative motion risk factor for post-operative arthrofibrosis
- younger, more active patients (reduces the incidence of meniscal or chondral injury)
- children (activity limitation is not realistic)
- older active patients (age >40 is not a contraindication if high demand athlete)
- partial/single bundle tears with clinical and functional instability
- prior ACL reconstruction failure
- high grade pivot test positive
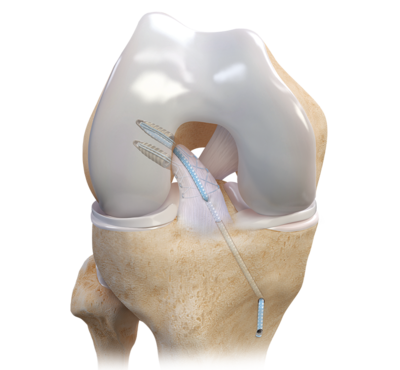
Primary ACL Repair: This technique is used in all age groups only if the injury is fresh. If it is a case of delayed treatment, the surgeon goes for other repair options. It is done arthroscopically; torn ligament is repaired back to its foot print with the help of suture anchors.
ACL repair procedure is a promising surgical alternative for acute ACL tears. Main advantage of the ACL repair is maintaining the natural proprioceptive receptors of the ligament. We prefer FiberTape internal bracing which works as an additional stabilizer following repair. It allows rapid rehabilitation and returning back to sports, helps patient to regain his confidence back early.
ACL Augmentation: The ACL has two bundles: anteromedial bundle and posterolateral bundle. This technique is suitable if only one of the bundles of the ligament is torn. A Hamstring tendon is harvested and ACL augmentation is done using harvested tendon. We always prefer to use FiberTape internal bracing in addition to graft. This will provide additional stability to graft which leads to excellent tendon and bone healing.
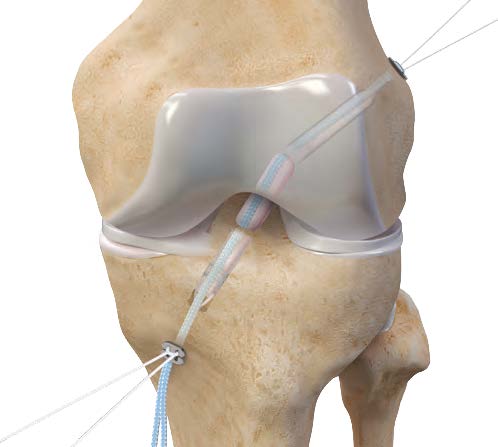
ACL Reconstruction: As the name suggests, in this procedure, the torn ligament is removed and a new one is reconstructed from another graft, generally the hamstring tendon is used as graft.
It is done using regional anesthesia, which makes it a painless procedure. Patient will be awake during this procedure, sometimes patient will be allowed to watch procedure through monitor. Surgery is performed arthroscopically with key hole which makes this procedure cosmetically more acceptable. We practice All inside ACL reconstruction with FiberTape internal bracing technique. This is latest and becoming very popular now a days.
Click on the following link to know about advantages of internal bracing.
https://www.youtube.com/watch?v=rEkCFKLF1uE&t=13s

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
