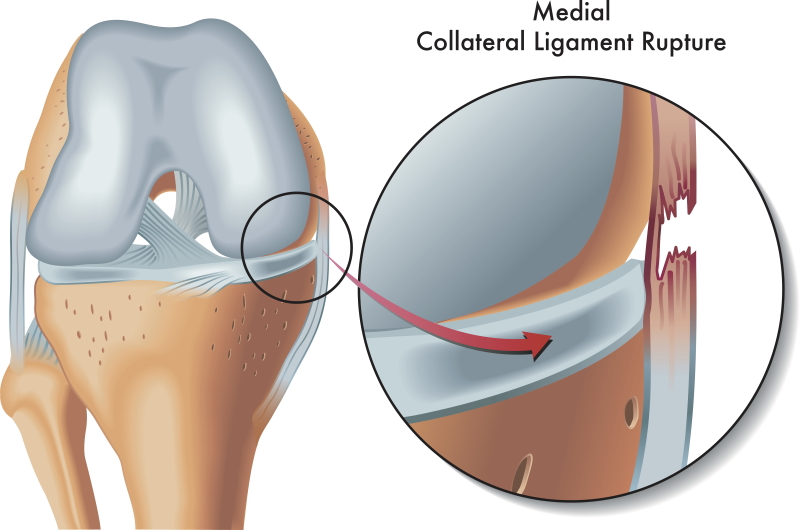
MCL (Medial collateral ligament) injury
MCL stands for Medial Collateral Ligament. It is one of the four ligaments that connect the femur (thigh bone) to the tibia (leg bone).
It has 2 layers
- Superficial MCL
- Deep MCL
Superficial layer is located in layer II of the medial side of knee. Superficial MCL originates on the medial epicondyle and inserting 7 to 10 cm below the joint line on the posterior half of the medial surface of the tibial metaphysis deep to the pes anserinus tendons.
Deep MCL is located in layer III of the medial knee. It blends with capsule and appears as the thickened part of it.
Functions:
Superficial MCL is primary stabilizer to valgus stress at all angles of knee flexion, but maximum contribution to stability is at 25 degrees knee flexion.
It also acts as secondary stabilizer to tibial external rotation and anterior/posterior tibial translation.
Deep MCL is secondary stabilizer to valgus stress and provide greatest stability contribution at full knee extension.
A medial collateral ligament (MCL) knee injury is a traumatic knee injury that typically occurs as a result of a sudden valgus force to the lateral aspect of the knee. Males are more commonly affected than females. Commonly occur in athletes account of 8% of all athletic knee injuries. Players of skiing, rugby, football, soccer and ice hockey have highest risk of MCL injury.
Etiology
Valgus stress is the most common mechanism of injury, usually with the knee held in slight flexion and external rotation.
Contact injury is more common than noncontact type, direct blow to the lateral knee with valgus force more often result in high grade / complete ligament disruption than noncontact injury. Rupture most commonly occurs at the femoral insertion of the MCL. Proximal MCL tears have greater healing rates than distal MCL tears which show inferior healing and residual valgus laxity.
Noncontact injuries are less common than contact but more common in skiing, pivoting or cutting activities with valgus and external rotation force. This more often result in low grade / incomplete ligament injury.
Anterior cruciate ligament (ACL) tear is most common associated injury with MCL. Combined ACL-MCL is the most common multiligamentous knee injury.
Presence of hemarthrosis is highly suggestive and often associated with high grade MCL injuries.
Classification:
American Medical Association (AMA) Classification – Based on joint laxity alone (described in 1966). Valgus stress applied with the knee in 30 degrees of flexion grading of injury done clinically based on the amount of medial joint line opening.
Less than 3 mm considered physiologic laxity which is considered as normal.
- Grade I injury: 3-5 mm joint opening on valgus stress test
- Grade II injury: 6-10 mm joint opening on valgus stress test
- Grade III injury: more than 10 mm joint opening on valgus stress test
Hughston Modification of the AMA Classification
It is based on joint laxity and injury severity: Severity graded by the extent of tenderness and quality of the endpoint with valgus stress at 30 degrees of knee flexion.
Grade I – Mild, First-degree injury, Firm endpoint with no joint laxity. It occurs as a result of stretch injury or only few MCL fibers are torn with no significant loss of ligament integrity.
Grade II – Moderate, Second-degree injury. It indicates incomplete or partial MCL tear. There is firm endpoint with mild increase in joint laxity of stress test.
Grade III – Severe, Third-degree injury. There is Complete MCL tear with no endpoint with valgus stress.
Presentation:
Patient gives history of forceful valgus stress which may occur as a result of blow on lateral side of knee. Patient may report a “pop” heard at time of injury
Symptoms:
- Pain and tenderness over medial joint line is most important symptoms.
- May have difficulty ambulating due to pain or instability
- Signs and symptoms of other associated injury may be present
- Knee effusion
Physical examination:
Valgus stress testing at 30° knee flexion isolates the superficial MCL. Medial gapping as compared to opposite knee indicates grade of injury
Valgus stressing at 0° knee extension, medial laxity with valgus stress indicates posteromedial capsule or cruciate ligament injury.
Imaging
Radiographs are recommended for MCL injury. AP, lateral and optional views like stress radiographs in skeletally immature patient may indicate gapping through physeal fracture.
In adults x-rays are usually normal. Very old MCL tears may show calcification at the medial femoral insertion site (Pellegrini-Stieda Syndrome).

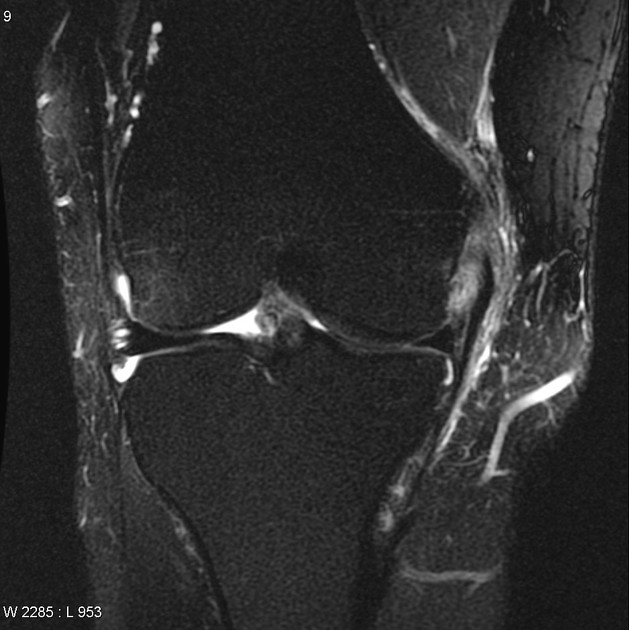
MRI: it is the best modality of choice for MCL injuries. Helps in locating and to know the extent of injury. We, the team cruciates recommend 3 tesla MRI for sports injuries because it gives better images, which helps in diagnostic accuracy so that we can provide better care.
Treatment Options:
Nonoperative
Isolated Grade I and II MCL injuries can be managed nonoperatively. Patient should not have any kind of instability for nonoperative management. Grade II injury with instability is indication for surgery.
Nonoperative management includes protected weight bearing and rehabilitation. Rest, icing, anti-inflammatory drugs, hinged knee braces can used as needed.
For Grade I injuries, quad sets, SLRs, and hip adduction above the knee to begin immediately. Cycling and progressive resistance exercises are started as tolerated. If everything goes in right direction an athlete should be able to return sports by 2 weeks.
Grade II tears need little longer time to return to sports.
Operative
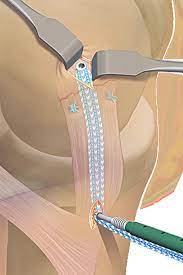
Primary MCL repair
This technique is used in all age groups only if the injury is fresh.Torn ligament is repaired back to its foot print with the help of suture anchors. We prefer to repair MCL with FiberTape internal bracing. MCL repair procedure is a promising surgical alternative for acute MCL tears. FiberTape internal bracing which works as an additional stabilizer following repair. It allows rapid rehabilitation and returning back to sports, helps patient to regain his confidence back early.
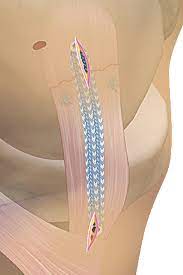
MCL reconstruction
It is done in case of chronic MCL injury with instability and in acute cases with loss of adequate tissue for repair. Diagnostic arthroscopy recommended for all surgical candidates to rule out associated injuries. It is an extra-articular procedure. We prefer one hamstring graft with FiberTape as internal brace for MCL reconstruction.
During old days, before introduction of internal brace techniques for the ligament reconstruction and repair surgery was done using a larger incision on the medial side of the knee. This increased the morbidity due knee stiffness and postoperative scar was not cosmetic. It needed a longer time for recovery and return to sports.
Now with introduction of the FiberTape internal brace, we perform MCL reconstruction and repair using percutaneous keyhole incisions and the Fiber tape internal bracing results in early mobilization of the knee following surgical procedure. Less pain, very minimal intraoperative blood loss, least chances of post-operative stiffness are the other advantages of this procedure.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}