Reverse Shoulder Arthroplasty
Introduction
This is a rather unusual and interesting solution to the rotator cuff tear arthropathy. In this method, the ball & socket are switched around so that the glenoid socket is converted into ball and the humeral head is converted into the socket.
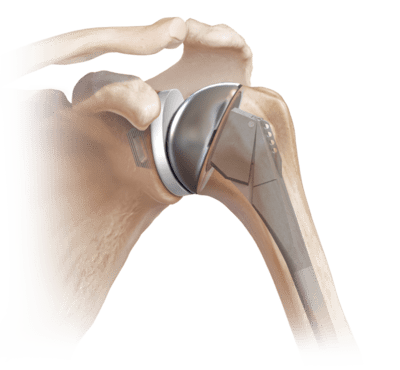
Mechanics behind this modification is center of rotation is moved inferiorly and is medialized. This allows the deltoid muscle to act on a longer fulcrum and have more mechanical advantage. Therefore, this surgery requires fully functional deltoid muscle as prerequisite.
Popularized in Europe and now increasingly used in North America. Now a days, it is getting popularity in India too.
Indications
- Rotator cuff tear arthropathy.
- Massive rotator cuff tear with pseudo paralysis.
- Massive rotator cuff tear with glenohumeral arthritis.
- Failed shoulder arthroplasty
- Rheumatoid arthritiswith adequate glenoid bone stock.
- Three or four part proximal humerus fractures in elderly older than 70 years of age.
- Re-implantation after tumour excision.
- Following periprosthetic fractures
- Non-union or mal-union of the tuberosity fractures of proximal humerus.
Patient characteristics (in clinical conditions above)
Low functional demand patients, physiological age >70
Pre requisites for Reverse Shoulder Arthroplasty
Sufficient glenoid bone stock. Working deltoid muscle. Intact axillary nerve
Contraindications
Deltoid deficiency (axillary nerve palsy). Bony acromion deficiency. Glenoid osteoporosis. Active infection
Biomechanics
The advantage of a reverse shoulder arthroplasty is that the center of rotation (COR) is moved inferiorly and medialized. This allows the deltoid muscle to act on a longer fulcrum and have more mechanical advantage to substitute for the deficient rotator cuff muscles to provide shoulder abduction and also allows increased shoulder abduction.
Does not significantly help shoulder internal or external rotation.
Reverse shoulder arthroplasty can be combined with latissimus dorsi transfer to assist with external rotation.
Surgical Technique
Approaches used-
Superolateral –
Lower incidence of postoperative instability. Lower risk of intraoperative scapular spine and acromion fractures
Deltopectoral-
Better preservation of active external rotation. Better orientation of glenoid component. Decreased risk of glenoid loosening and scapular notching.
Technique
Humeral preparation – Humeral head typically osteotomized anywhere between 0 and 30 degrees of retroversion. More retroversion is gaining popularity as it may improve post-op external rotation, long head of biceps is tenotomised, reaming and broaching of humerus is done.
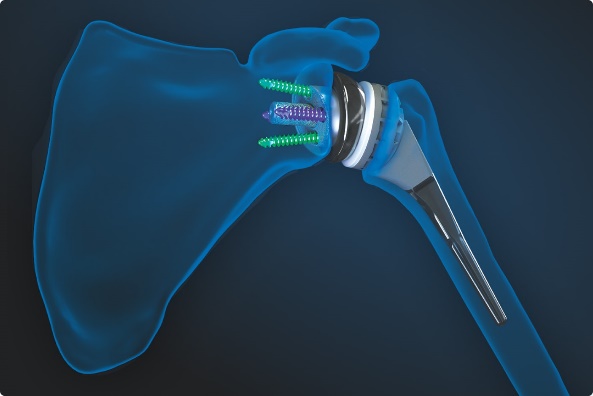
Glenoid preparation – Labrum is excised and capsule is released circumferentially, place baseplate as inferiorly as possible with an inferior tilt, mount glenosphere onto baseplate.
Tuberosity repair – Anatomic repair of the greater tuberosity is done. It is associated with improved shoulder external rotation, function and patient satisfaction compared to tuberosity resection.
Complications
Infection
Humeral fractures, glenoid fractures or perforations during surgery
Instability
Loosening
Scapular notching
Dislocations



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}