SHOULDER IMPINGEMENT
There are 2 main causes of impingement in shoulder :
 Clinically provisional diagnosis is made on the basis of physical examination supported with a positive Neer impingement and Hawkins tests and is confirmed with MRI.
Initial treatment is always a trial of nonsurgical measures which includes NSAIDs, physical therapy and corticosteroid injections. Arthroscopic subacromial decompression with or without acromioplasty is done in patients who fail to improve with nonsurgical modalities.
Causes and Pathophysiology of Subacromial impingement
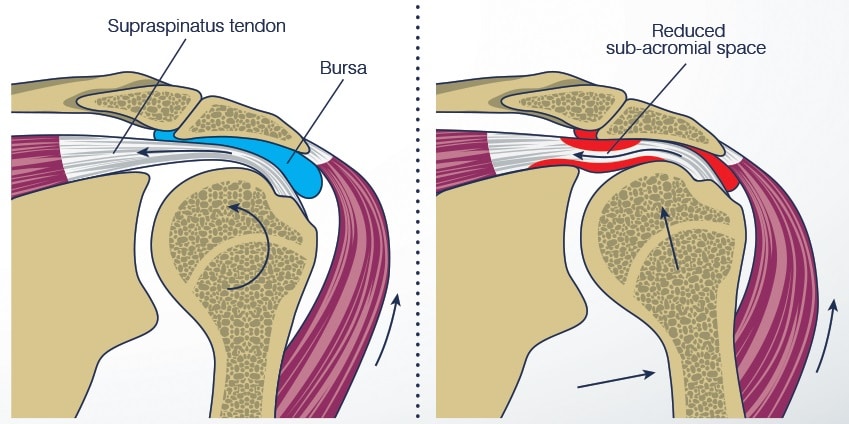
Subacromial impingement occurs due to combination of extrinsic compression of the rotator cuff muscles between the humeral head andanterior part of acromion, coracoacromial ligaments, and acromioclavicular joint. Because of this compression there is intrinsic degeneration of supraspinatus muscle which results in imbalance of humeral head which in turn results in proximal migration, as a result of this narrowing of subacromial space occurs.
Narrowing of subacromial space results in inflammation of the subacromial bursa because of compression between the humeral head with rotator cuff, acromion and associated structures.
Subacromial impingement is always first stage of rotator cuff pathology which occurs as a result of impingement resulting in partial to full-thickness tear in future.
Predisposing conditions which lead to Subacromial impingement are
Clinically provisional diagnosis is made on the basis of physical examination supported with a positive Neer impingement and Hawkins tests and is confirmed with MRI.
Initial treatment is always a trial of nonsurgical measures which includes NSAIDs, physical therapy and corticosteroid injections. Arthroscopic subacromial decompression with or without acromioplasty is done in patients who fail to improve with nonsurgical modalities.
Causes and Pathophysiology of Subacromial impingement
Subacromial impingement occurs due to combination of extrinsic compression of the rotator cuff muscles between the humeral head andanterior part of acromion, coracoacromial ligaments, and acromioclavicular joint. Because of this compression there is intrinsic degeneration of supraspinatus muscle which results in imbalance of humeral head which in turn results in proximal migration, as a result of this narrowing of subacromial space occurs.
Narrowing of subacromial space results in inflammation of the subacromial bursa because of compression between the humeral head with rotator cuff, acromion and associated structures.
Subacromial impingement is always first stage of rotator cuff pathology which occurs as a result of impingement resulting in partial to full-thickness tear in future.
Predisposing conditions which lead to Subacromial impingement are

 Technique –
Technique –
 Initial treatment is always a course of conservative measures which includes NSAIDs, physiotherapy and corticosteroid injections. Surgery is indicated for patients who fail to respond to nonoperative measures.
Etiology:
Patients with congenital bone pathologies like long or more lateral placed coracoid process.
Previous surgery that resulted in posterior capsular tightening can cause impingement. Maximal impingement is seen when arm is in adduction, flexion, and internal rotation.
Associated conditions are combined subscapularis, supraspinatus, and infraspinatus tears.
Symptoms and presentation
Pain over the anterior shoulder. Pain gets worse when shoulder is brought to adduction, flexion and internal rotation.
Physical exam: tenderness elicited over anterior coracoid. Maximum pain is seen at 120-130° of arm flexion and internal rotation
Imaging
Initial treatment is always a course of conservative measures which includes NSAIDs, physiotherapy and corticosteroid injections. Surgery is indicated for patients who fail to respond to nonoperative measures.
Etiology:
Patients with congenital bone pathologies like long or more lateral placed coracoid process.
Previous surgery that resulted in posterior capsular tightening can cause impingement. Maximal impingement is seen when arm is in adduction, flexion, and internal rotation.
Associated conditions are combined subscapularis, supraspinatus, and infraspinatus tears.
Symptoms and presentation
Pain over the anterior shoulder. Pain gets worse when shoulder is brought to adduction, flexion and internal rotation.
Physical exam: tenderness elicited over anterior coracoid. Maximum pain is seen at 120-130° of arm flexion and internal rotation
Imaging
- Subacromial impingement
- Subcoracoid Impingement
Clinically provisional diagnosis is made on the basis of physical examination supported with a positive Neer impingement and Hawkins tests and is confirmed with MRI.
Initial treatment is always a trial of nonsurgical measures which includes NSAIDs, physical therapy and corticosteroid injections. Arthroscopic subacromial decompression with or without acromioplasty is done in patients who fail to improve with nonsurgical modalities.
Causes and Pathophysiology of Subacromial impingement
Subacromial impingement occurs due to combination of extrinsic compression of the rotator cuff muscles between the humeral head andanterior part of acromion, coracoacromial ligaments, and acromioclavicular joint. Because of this compression there is intrinsic degeneration of supraspinatus muscle which results in imbalance of humeral head which in turn results in proximal migration, as a result of this narrowing of subacromial space occurs.
Narrowing of subacromial space results in inflammation of the subacromial bursa because of compression between the humeral head with rotator cuff, acromion and associated structures.
Subacromial impingement is always first stage of rotator cuff pathology which occurs as a result of impingement resulting in partial to full-thickness tear in future.
Predisposing conditions which lead to Subacromial impingement are
- Shape of the acromion
- osacromiale
- contracture of posterior capsule
- scapular dyskinesia
- malunited tuberosity fractures
- Type I – Flat
- Type II – Curved
- Type III – Hooked, Type III is most commonly associated with Subacromial impingement.
- Positive Neer’s impingement sign
- Neer’s impingement test:
- Hawkin-Kennedy test
- Radiographs
- True AP view of the shoulder (Grashey view): it is very useful in accessing the acromiohumeral interval. Normally it is between 7-14 mm. anything less than this predisposes to impingement.
- 30° caudal tilt view: this is a useful view in determining subacromial spurring.
- supraspinatus outlet view: very useful in accessing acromial morphology
- MRI
- CT arthography
- Ultrasound
- Nonoperative
- It is always used as first line and mainstay of treatment of isolated subacromial impingement. When it is associated with rotator cuff tear subacromial steroid injection is not indicated.
- Physiotherapy includes rotator cuff strengthening exercises and periscapular muscle strengthening and stabilization protocol.
- Operative
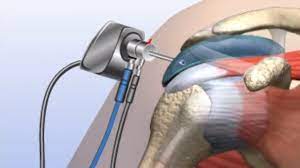
Technique –
- surgery is performed under general anesthesia
- lateral or beech chair position is used
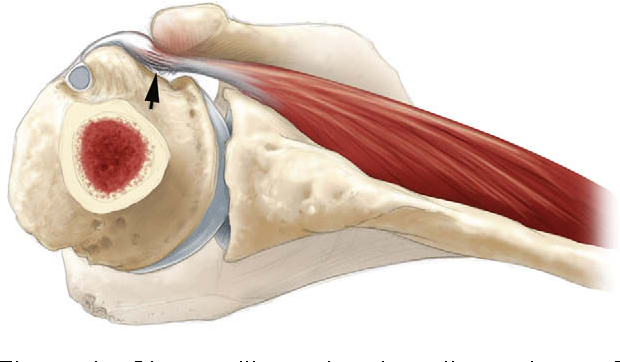
- first anterior acromionectomy is performed
- the anterior deltoid origin determines the extent of the acromionectomy and it must remain intact.
- Is outdated and not being used now a days.
Initial treatment is always a course of conservative measures which includes NSAIDs, physiotherapy and corticosteroid injections. Surgery is indicated for patients who fail to respond to nonoperative measures.
Etiology:
Patients with congenital bone pathologies like long or more lateral placed coracoid process.
Previous surgery that resulted in posterior capsular tightening can cause impingement. Maximal impingement is seen when arm is in adduction, flexion, and internal rotation.
Associated conditions are combined subscapularis, supraspinatus, and infraspinatus tears.
Symptoms and presentation
Pain over the anterior shoulder. Pain gets worse when shoulder is brought to adduction, flexion and internal rotation.
Physical exam: tenderness elicited over anterior coracoid. Maximum pain is seen at 120-130° of arm flexion and internal rotation
Imaging
- Radiographs: shows reduced coracohumeral distance.
- CT scan:
- This is done with arms crossed over chest
- coracohumeral distance of less than 6 mm is abnormal finding
- normally coracohumeral distance is around 8.5 mm with arm adducted and 6.5 mm with arm in flexion.
- MRI:
- This is used to access soft tissue pathology
- it shows increased signal at subscapularis muscle, sometimes may show complete tear with subluxation of biceps tendon.
- axial view can be used measure coracohumeral distance.
- Nonoperative
- It is always used as first line and mainstay of treatment of isolated subcorocoid impingement. When it is associated with rotator cuff tear subacromial steroid injection is not indicated.
- Physiotherapy includes stretching exercises and periscapular muscle strengthening and stabilization protocol.
- Operative
- surgery is performed under general anesthesia
- lateral or beech chair position is used
- Resection of posterolateral part of coracoid to create a 7 mm of coracohumeral distance.
- If there is significant subscapularis tendon tear then it has to be repaired.
- Is outdated and not being used now a days because of advancement in arthroscopic procedures.
- Resection of lateral aspect of coracoid process and the conjoined tendon is reattached to the remaining coracoid.
After suffering from ACL injury, I have always been in lot of pain and instability. I was going to give up on playing football but since I got my treatment done by Dr Nagendra Prasad I am back on the field with full confidence.
rakesh kumar 
Dr Prasad is the best surgeon I have ever met. Seriously, the guy is genius and has hands of gold. I can’t thank him enough for how he helped me when I was at my worst time after sustaining ligament injury.
Minakshi Tomar

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}